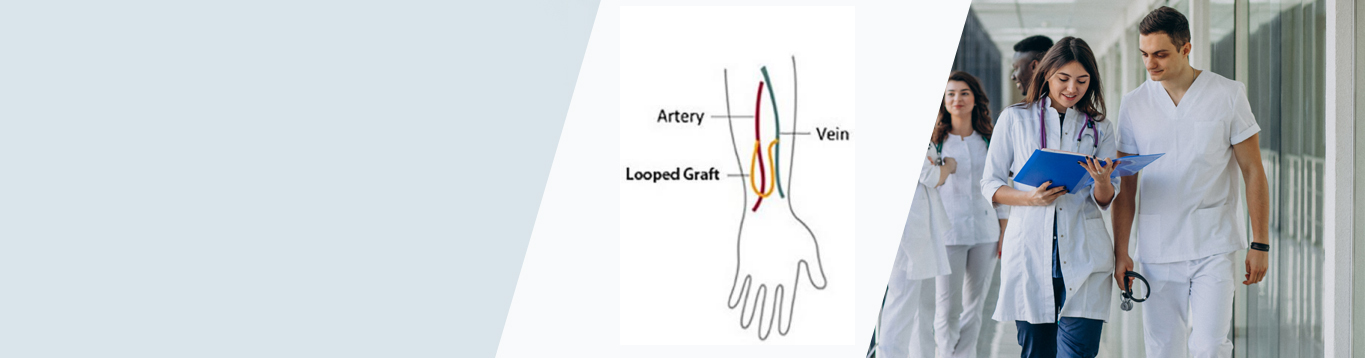
The function of the veins is to take the de-oxygenated blood from the periphery/ various organs of the body and take it back to the heart/ lung for oxygen on. Veins are thin walled tubes that we commonly see on the back of our hands or on feet.
Veins are present all over the body. The veins in the just below the skin are called Superficial veins. There is another set of larger veins that runs deep between the muscles of the legs, abdomen, arms, neck etc. these veins are called Deep Veins.

All of these veins have valves that permit
unidirectional flow of blood from the periphery to the heart.
The most common diseases of the veins
involve either a failure of these valves or
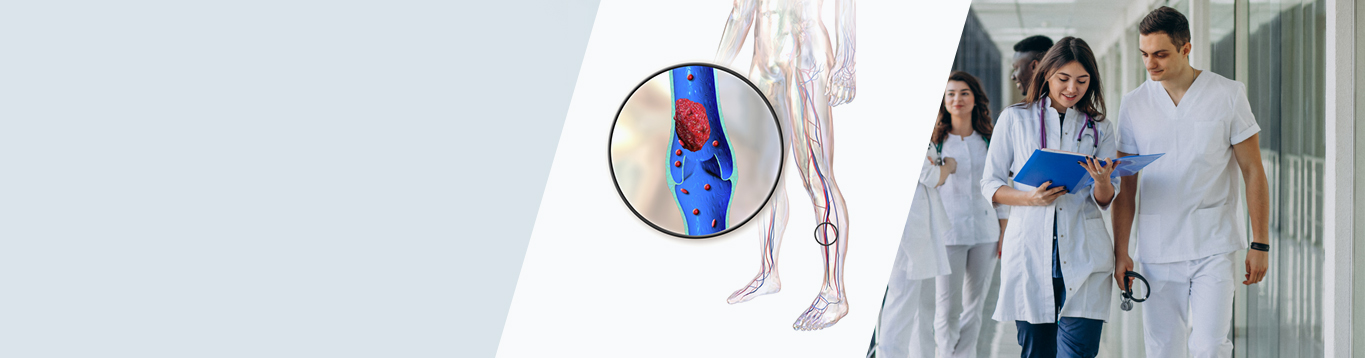
clotting of blood in these veins. Varicose veins is a condition that arises from failure of valves that can happen due to a variety of reasons.
Varicose veins is probably the most common venous disease. Similarly, clotting of blood in the veins is known as Venous Thrombosis. This clotting or thrombosis can happen in any of the veins, but is frequently seen after i.v. injections. Occasionally though, this clotting can happen in the deep venous segments of the leg, known as Deep Vein Thrombosis (DVT)
DVT is a potentially lethal disease as these
clots can migrate to the lungs and can be life threatening in the acute stage and lifestylethreatening in the chronic stage.